Summit Therapeutics Reports Financial Results and Operational Progress for the First Quarter Ended March 31, 2024
HARMONi and HARMONi-3 Enrollment Continues
Promising Intracranial Anti-Tumor Activity and Safety Data Featured at the 2024 European Lung Cancer Congress with Ivonescimab Alone or Combined with Chemotherapy Achieving 34% Intracranial Responses;
Median Intracranial PFS of 19.3 months in NSCLC Patients with Brain Metastases
Board of Directors Strengthened with the Addition of Dr. Mostafa Ronaghi
Updated Guidance of Cash Runway for Operations through Q1 2025
Miami, Florida, May 1, 2024 – Summit Therapeutics Inc. (NASDAQ: SMMT) (“Summit,” “we,” or the “Company”) today reports its financial results and provides an update on operational progress for the first quarter ended March 31, 2024.
Operational & Corporate Updates
- Our operational progress continues with ivonescimab (SMT112), an investigational, potentially first-in-class bispecific antibody combining the effects of immunotherapy via a blockade of PD-1 with the anti-angiogenesis effects associated with blocking VEGF into a single molecule:
- January 2024 marked the one-year anniversary of the close of our Collaboration and License Agreement with Akeso Inc. (Akeso) for ivonescimab (SMT112), with which over 1,600 have been treated in clinical studies globally. Summit received rights to develop and commercialize ivonescimab in the United States, Canada, Europe, and Japan, while Akeso retains development and commercialization rights for the rest of the world, including China. Since in-licensing ivonescimab, we launched late-stage clinical development in non-small cell lung cancer (NSCLC) and are actively enrolling two registrational Phase III trials in the following proposed indications:
- HARMONi Phase III Trial: Ivonescimab combined with chemotherapy in patients with epidermal growth factor receptor (EGFR)-mutated, locally advanced or metastatic non-squamous NSCLC who have progressed after treatment with a third-generation EGFR tyrosine kinase inhibitor (TKI), with enrollment completion expected in the second half of 2024, and
- HARMONi-3 Phase III Trial: Ivonescimab combined with chemotherapy in first-line metastatic squamous NSCLC patients, with the first patient having been treated in the fourth quarter of 2023
- In January 2024, followed by a presentation at ELCC 2024 in March 2024, Akeso announced updates from its Phase II AK112-201 trial data. Notably, in patients with first line advanced or metastatic squamous NSCLC without actionable genomic alterations (Cohort 1, n=63), a median PFS (mPFS) of 11.1 months (95% CI: 9.5 – 16.3 months) was observed; median overall survival (mOS) was not yet reached after a median follow-up time of 22.1 months. Additionally, in patients with advanced or metastatic NSCLC whose tumors are positive for EGFR mutations and have progressed following an EGFR TKI (Cohort 2, n=19), mPFS of 8.5 months (95% CI: 4.1 – 12.9 months) was observed, and a mOS of 22.5 months (95% CI: 10.4 – NE) was achieved after a median follow-up time of 25.8 months. Treatment-related adverse events leading to discontinuation of ivonescimab was 11% and 0% in the two populations, respectively; there were no treatment-related adverse events leading to a patient’s death in either setting. AK112-201 is a study of Chinese subjects receiving ivonescimab plus chemotherapy conducted and analyzed by our partners, Akeso, of which the updated data supports Summit’s HARMONi and HARMONi-3 Phase III clinical trials.
- Also at ELCC 2024, Summit and Akeso highlighted promising ivonescimab Phase II data in NSCLC patients with brain metastases. The analysis consisted of 35 patients with advanced or metastatic NSCLC who had asymptomatic brain metastases at baseline and received ivonescimab alone or in combination with chemotherapy. Across all patients analyzed, an intracranial response rate of 34% was achieved, including 23% complete responses, by response assessment in neuro-oncology (RANO) criteria and median intracranial progression-free survival was 19.3 months. All patients who did not achieve a response demonstrated stable disease or non-progression; no patients experienced intracranial disease progression at the time of the initial follow-up scan. No cases of intracranial bleeding complications were observed in these patients. The data was from patients participating in AK112-201, described above, or AK112-202, in which ivonescimab was delivered as monotherapy.
- In April 2024, the Company appointed Mostafa Ronaghi, PhD, to its Board of Directors. Dr. Ronaghi is the Co-Founder and Executive Board Member of Cellanome. He was previously the Chief Technology Officer at Illumina, Inc. from 2008 to 2021. While at Illumina, in 2016, Dr. Ronaghi co-founded GRAIL, a next-gen liquid biopsy platform for cancer detection. Prior to Illumina, Dr. Ronaghi was Principal Investigator at the Stanford Genome Technology Center from 1999 to 2008. Throughout his prolific career, Dr. Ronaghi co-founded several companies which sought to increase the understanding of particular diseases through next-generation sequencing (NGS), advanced genotyping, or other advanced technology. Dr. Ronaghi holds a Ph.D. in Biotechnology from Royal Institute of Technology in Stockholm, Sweden.
- January 2024 marked the one-year anniversary of the close of our Collaboration and License Agreement with Akeso Inc. (Akeso) for ivonescimab (SMT112), with which over 1,600 have been treated in clinical studies globally. Summit received rights to develop and commercialize ivonescimab in the United States, Canada, Europe, and Japan, while Akeso retains development and commercialization rights for the rest of the world, including China. Since in-licensing ivonescimab, we launched late-stage clinical development in non-small cell lung cancer (NSCLC) and are actively enrolling two registrational Phase III trials in the following proposed indications:
Financial Highlights
Cash and Cash Equivalents, Restricted Cash, & Short-term Investments
- Aggregate cash and cash equivalents, restricted cash, and short-term investments were $157.0 million and $186.2 million at March 31, 2024 and December 31, 2023, respectively. Research and development tax credits were $1.2 million and $1.8 million at March 31, 2024 and December 31, 2023, respectively.
- Our short-term investments consist of U.S. treasury securities.
- Operating cash outflow for the three months ended March 31, 2024 and 2023 was $30.1 million and $13.1 million, respectively.
GAAP and Non-GAAP Research and Development (R&D) Expenses
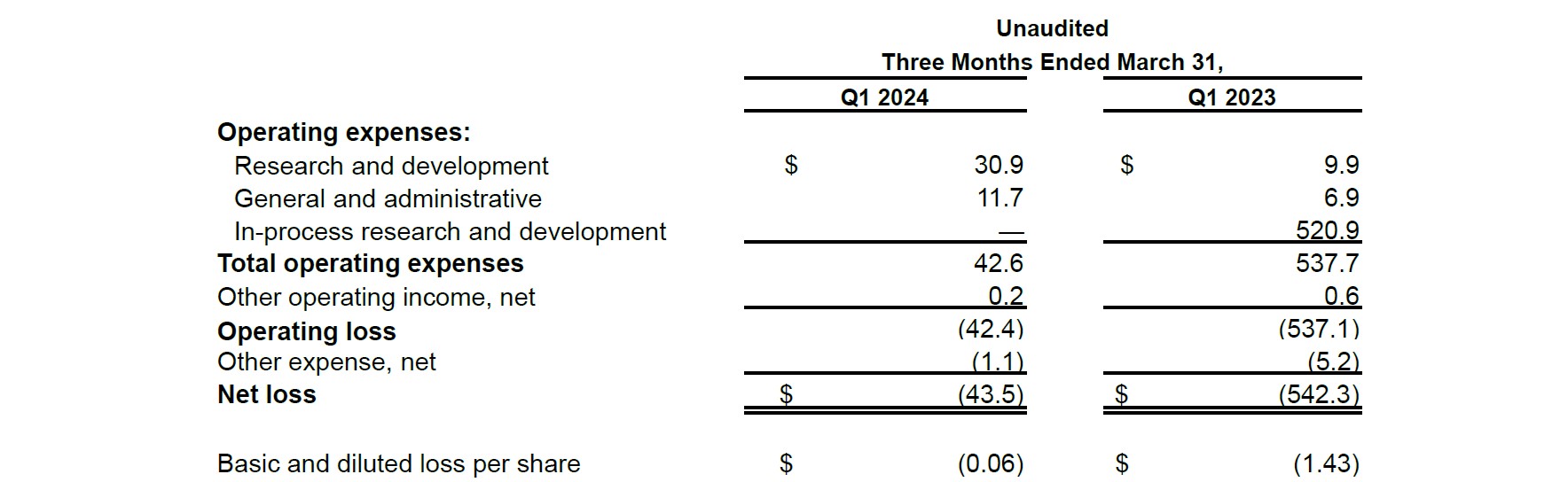
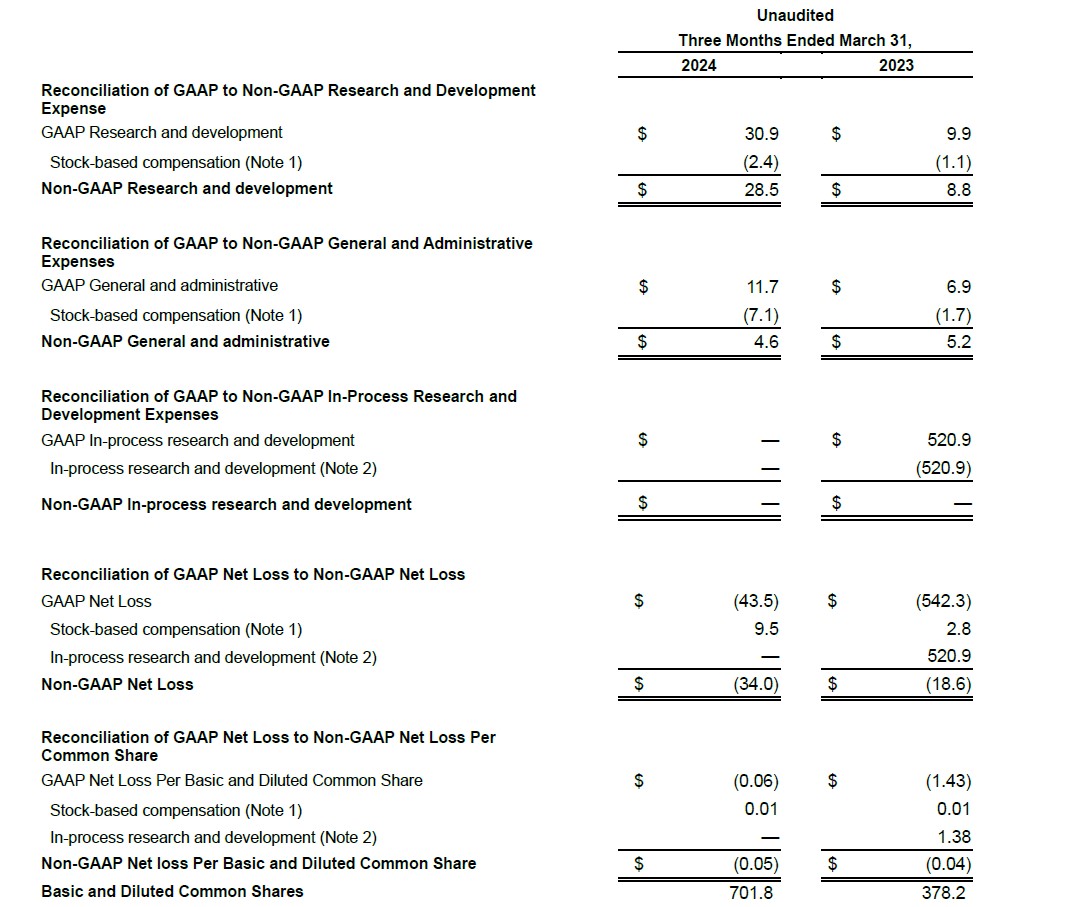
- R&D expenses according to generally accepted accounting principles in the U.S. (“GAAP”) were $30.9 million for the first quarter of 2024, compared to $9.9 million for the same period of the prior year.
- Non-GAAP R&D expenses were $28.5 million for the first quarter of 2024, compared to $8.8 million for the same period of the prior year.
GAAP and Non-GAAP General and Administrative (G&A) Expenses
- GAAP G&A expenses were $11.7 million for the first quarter of 2024, compared to $6.9 million for the same period of the prior year.
- Non-GAAP G&A expenses were $4.6 million for the first quarter of 2024, compared to $5.2 million for the same period of the prior year.
GAAP and Non-GAAP Operating Expenses
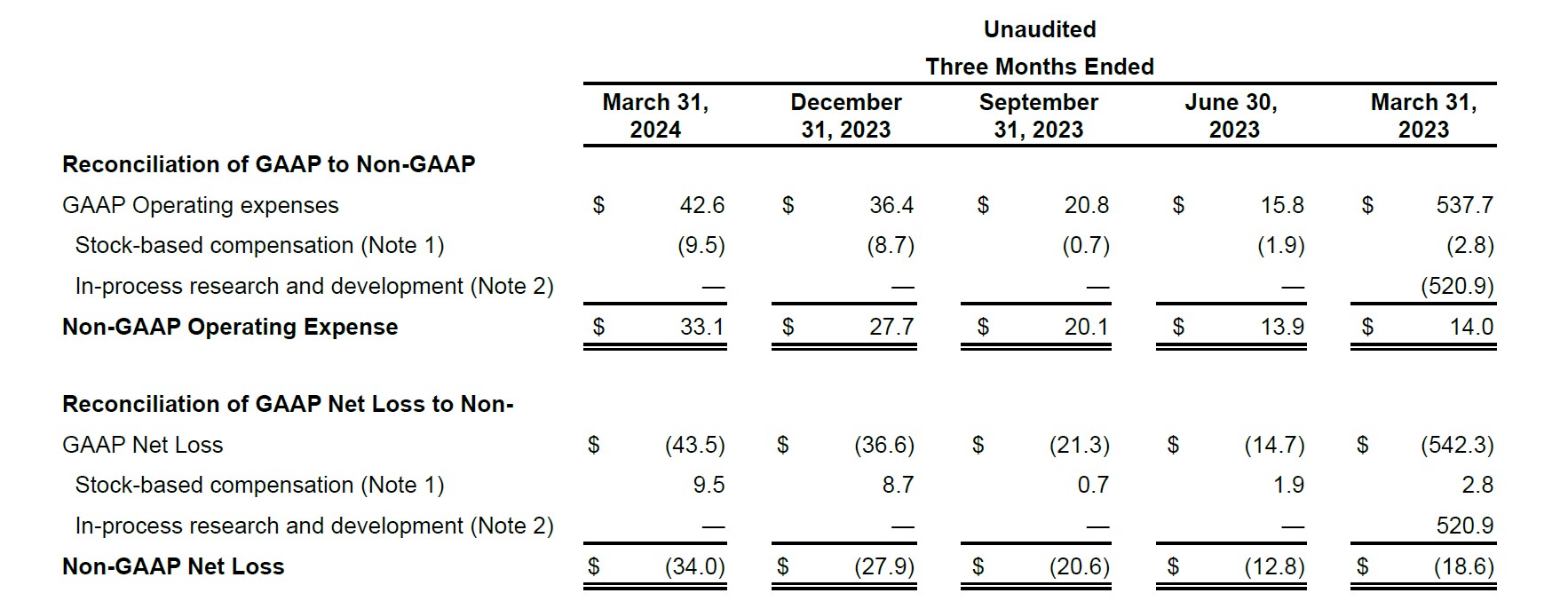
- GAAP operating expenses were $ 42.6 million for the first quarter of 2024, compared to $537.7 million for the same period of the prior year. First quarter 2023 GAAP operating expenses included $520.9M in- process research and development expense that was primarily related to our upfront milestone payments pursuant to the License Agreement with Akeso.
- Non-GAAP operating expenses were $33.1 million for the first quarter of 2024, compared to $14.0 million for the same period of the prior year. The increase is primarily due to expansion of clinical study and development costs related to ivonescimab and increases in people cost as we continue to build out our R&D team.
GAAP and Non-GAAP Net Loss
- GAAP net loss in the first quarter of 2024 and 2023 was $43.5 million or $0.06 per basic and diluted share, and $542.3 million or $1.43 per basic and diluted share, respectively.
- Non-GAAP net loss in the first quarter of 2024 and 2023 was $34.0 million or $0.05 per basic and diluted share, and $18.6 million or $0.04 per basic and diluted share, respectively.
Use of Non-GAAP Financial Results
This release includes measures that are not in accordance with U.S. generally accepted accounting principles (“Non-GAAP measures”). These Non-GAAP measures should be viewed in addition to, and not as a substitute for, Summit’s reported GAAP results, and may be different from Non-GAAP measures used by other companies. In addition, these Non-GAAP measures are not based on any comprehensive set of accounting rules or principles. Summit management uses these non-GAAP measures for internal budgeting and forecasting purposes and to evaluate Summit’s financial performance. Summit management believes the presentation of these Non-GAAP measures is useful to investors for comparing prior periods and analyzing ongoing business trends and operating results. For further information regarding these Non-GAAP measures, please refer to the tables presenting reconciliations of our Non-GAAP results to our U.S. GAAP results and the “Notes on our Non- GAAP Financial Information” at the end of this press release.
First Quarter 2024 Earnings Call
Summit will host an earnings call this morning, Wednesday, May 1, 2024, at 9:00am ET. The conference call will be accessible by dialing (888) 210-3702 (toll-free domestic) or (646) 960-0191 (international) using conference code 5785899. A live webcast and instructions for joining the call are accessible through Summit’s website www.smmttx.com. An archived edition of the webcast will be available on our website after the call.
About Ivonescimab
Ivonescimab, known as SMT112 in Summit’s license territories, the United States, Canada, Europe, and Japan, and as AK112 in China and Australia, is a novel, potential first-in-class investigational bispecific antibody combining the effects of immunotherapy via a blockade of PD-1 with the anti-angiogenesis effects associated with blocking VEGF into a single molecule. Ivonescimab displays unique cooperative binding to each of its intended targets with higher affinity when in the presence of both PD-1 and VEGF.
This could differentiate ivonescimab as there is potentially higher expression (presence) of both PD-1 and VEGF in tumor tissue and the tumor microenvironment (TME) as compared to normal tissue in the body. Ivonescimab’s tetravalent structure (four binding sites) enables higher avidity (accumulated strength of multiple binding interactions) in the tumor microenvironment with over 18-fold increased binding affinity to PD-1 in the presence of VEGF in vitro, and over 4-times increased binding affinity to VEGF in the presence of PD-1 in vitro.1 This tetravalent structure, the intentional novel design of the molecule, and bringing these two targets into a single bispecific antibody with cooperative binding qualities have the potential to direct ivonescimab to the tumor tissue versus healthy tissue. The intent of this design, together with a half-life of 6 to 7 days,1 is to improve upon previously established efficacy thresholds, in addition to side effects and safety profiles associated with these targets.
Ivonescimab was discovered by Akeso Inc. (HKEX Code: 9926.HK) and is currently engaged in multiple Phase III clinical trials. Over 1,600 patients have been treated with ivonescimab in clinical studies globally. Summit has begun its clinical development of ivonescimab in non-small cell lung cancer (NSCLC), commencing enrollment in 2023 in two Phase III clinical trials, HARMONi and HARMONi-3.
HARMONi is a Phase III clinical trial which intends to evaluate ivonescimab combined with chemotherapy compared to a placebo plus chemotherapy in patients with EGFR-mutated, locally advanced or metastatic non- squamous NSCLC who have progressed after treatment with a third-generation EGFR TKI (e.g., osimertinib).
HARMONi-3 is a Phase III clinical trial which is designed to evaluate ivonescimab combined with chemotherapy compared to pembrolizumab combined with chemotherapy in patients with first-line metastatic squamous NSCLC.
Ivonescimab is an investigational therapy that is not approved by any regulatory authority

1 Zhong, et al, SITC 2023
About Lung Cancer
Lung cancer is believed to impact approximately 600,000 people across the United States, United Kingdom, Spain, France, Italy, Germany, and Japan.2 NSCLC is the most prevalent type of lung cancer and represents approximately 80% to 85% of all incidences.3 Among patients with non-squamous NSCLC, approximately 15% have EGFR-sensitizing mutations in the United States and Europe.4 Patients with squamous histology represent approximately 25% to 30% of NSCLC patients.5
2 American Cancer Society: www.cancer.org/cancer/types/lung-cancer/about/key-statistics.html (Accessed Jan 2024); World Health Organization: International Agency for Research on Cancer, Globocan data by country (UK, Spain, France, Italy, Germany); Japan National Cancer Registry.
3 Schabath MB, Cote ML. Cancer Progress and Priorities: Lung Cancer. Cancer Epidemiology, Biomarkers & Prevention. (2019).
4 About EGFR-Positive Lung Cancer | Navigating EGFR (lungevity.org)
5 Schabath MB, Cote ML. Cancer Progress and Priorities: Lung Cancer. Cancer Epidemiology, Biomarkers & Prevention. (2019).
About Summit Therapeutics
Summit Therapeutics Inc. is a biopharmaceutical oncology company focused on the discovery, development, and commercialization of patient-, physician-, caregiver- and societal-friendly medicinal therapies intended to improve quality of life, increase potential duration of life, and resolve serious unmet medical needs.
Summit was founded in 2003 and our shares are listed on the Nasdaq Global Market (symbol “SMMT”). We are headquartered in Miami, Florida, and we have additional offices in Menlo Park, California, and Oxford, UK.
For more information, please visit https://www.smmttx.com and follow us on X (formerly Twitter) @summitplc.
Contact Summit Investor Relations:
Dave Gancarz
Chief Business & Strategy Officer
Nathan LiaBraaten
Senior Director, Investor Relations
investors@smmttx.com
Summit Forward-looking Statements
Any statements in this press release about the Company’s future expectations, plans and prospects, including but not limited to, statements about the clinical and preclinical development of the Company’s product candidates, entry into and actions related to the Company’s partnership with Akeso Inc., the Company’s anticipated spending and cash runway, the therapeutic potential of the Company’s product candidates, the potential commercialization of the Company’s product candidates, the timing of initiation, completion and availability of data from clinical trials, the potential submission of applications for marketing approvals, potential acquisitions, and other statements containing the words “anticipate,” “believe,” “continue,” “could,” “estimate,” “expect,” “intend,” “may,” “plan,” “potential,” “predict,” “project,” “should,” “target,” “would,” and similar expressions, constitute forward-looking statements within the meaning of The Private Securities Litigation Reform Act of 1995. Actual results may differ materially from those indicated by such forward-looking statements as a result of various important factors, including the results of our evaluation of the underlying data in connection with the development and commercialization activities for ivonescimab, the outcome of discussions with regulatory authorities, including the Food and Drug Administration, the uncertainties inherent in the initiation of future clinical trials, availability and timing of data from ongoing and future clinical trials, the results of such trials, and their success, and global public health crises, that may affect timing and status of our clinical trials and operations, whether preliminary results from a clinical trial will be predictive of the final results of that trial or whether results of early clinical trials or preclinical studies will be indicative of the results of later clinical trials, whether business development opportunities to expand the Company’s pipeline of drug candidates, including without limitation, through potential acquisitions of, and/or collaborations with, other entities occur, expectations for regulatory approvals, laws and regulations affecting government contracts and funding awards, availability of funding sufficient for the Company’s foreseeable and unforeseeable operating expenses and capital expenditure requirements and other factors discussed in the “Risk Factors” section of filings that the Company makes with the Securities and Exchange Commission. Any change to our ongoing trials could cause delays, affect our future expenses, and add uncertainty to our commercialization efforts, as well as to affect the likelihood of the successful completion of clinical development of ivonescimab. Accordingly, readers should not place undue reliance on forward-looking statements or information. In addition, any forward-looking statements included in this press release represent the Company’s views only as of the date
of this release and should not be relied upon as representing the Company’s views as of any subsequent date. The Company specifically disclaims any obligation to update any forward-looking statements included in this press release.
Summit Therapeutics Inc.
GAAP Condensed Consolidated Statements of Operations
(in millions, except per share data)
Summit Therapeutics Inc.
GAAP Condensed Consolidated Balance Sheet Information
(in millions)

Summit Therapeutics Inc.
GAAP Condensed Consolidated Statement of Cash Flows Information
(in millions)

Summit Therapeutics Inc.
Schedule Reconciling Selected Non-GAAP Financial Measures
(in millions, except per share data)
Summit Therapeutics Inc.
Schedule Reconciling Selected Non-GAAP Financial Measures
(in millions)
Summit Therapeutics, Inc.
Notes on our Non-GAAP Financial Information
Non-GAAP financial measures adjust GAAP financial measures for the items listed below. These Non-GAAP measures should be viewed in addition to, and not as a substitute for Summit’s reported GAAP results, and may be different from Non-GAAP measures used by other companies. In addition, these Non-GAAP measures are not based on any comprehensive set of accounting rules or principles. Summit management uses these non-GAAP measures for internal budgeting and forecasting purposes and to evaluate Summit’s financial performance. Summit management believes the presentation of these Non-GAAP measures is useful to investors for comparing prior periods and analyzing ongoing business trends and operating results.
Each of non-GAAP Research and Development Expense, non-GAAP General and Administrative Expenses, non-GAAP Operating Expenses, Non-GAAP Net Loss and Non-GAAP EPS differ from GAAP in that such measures exclude the non-cash charges and costs associated with stock-based compensation. In addition, (i) non-GAAP In-Process Research and Development Expenses, non-GAAP Operating Expenses, non-GAAP Net Loss and non-GAAP EPS each exclude certain one-time charges associated with in-process research and development and (ii) non-GAAP In-Process Research and Development Expenses excludes certain in-process research and development charges, in each case as described further in the notes below and as expressed in the tabular reconciliation presented above.
Note 1: Stock-based compensation is a non-cash charge and costs calculated for this expense can vary year-over-year depending on the stock price of awards on the date of grant as well as the timing of compensation award arrangements.
Note 2: In-process research and development represents a one-time charge associated with the Company’s in-licensing of ivonescimab from Akeso.
Appendix: Glossary of Critical Terms Contained Herein
Affinity – Affinity is the strength of binding of a molecule, such as a protein or antibody, to another molecule, such as a ligand.
Avidity – Avidity is the accumulated strength of multiple binding interactions.
Angiogenesis – Angiogenesis is the development, formation, and maintenance of blood vessel structures. Without sufficient blood flow, tissue may experience hypoxia (insufficient oxygen) or lack of nutrition, which may cause cell death.6
Cooperative binding – Cooperative binding occurs when the number of binding sites on the molecule that can be occupied by a specific ligand (e.g., protein) is impacted by the ligand’s concentration. For example, this can be due to an affinity for the ligand that depends on the amount of ligand bound or the binding strength of the molecule to one ligand based on the concentration of another ligand, increasing the chance of another ligand binding to the compound.7
Immunotherapy – Immunotherapy is a type of treatment, including cancer treatments, that help a person’s immune system fight cancer. Examples include anti-PD-1 therapies.8
Intracranial – Within the cranium or skull.
PD-1 – Programmed cell Death protein 1 is a protein on the surface of T cells and other cells. PD-1 plays a key role in reducing the regulation of ineffective or harmful immune responses and maintaining immune tolerance. However, with respect to cancer tumor cells, PD-1 can act as a stopping mechanism (a brake or checkpoint) by binding to PD-L1 ligands that exist on tumor cells and preventing the T cells from targeting cancerous tumor cells.9
PD-L1 – Programmed cell Death Ligand 1 is expressed by cancerous tumor cells as an adaptive immune mechanism to escape anti-tumor responses, thus believed to suppress the immune system’s response to the presence of cancer cells. 10
PD-L1 TPS – PD-L1 Tumor Proportion Score represents the percentage of tumor cells that express PD-L1 proteins.
PFS – Progression-Free Survival.
RANO – Response Assessment in Neuro-Oncology, the standard for assessing the response of a brain or spinal cord tumor to therapy.
SQ-NSCLC – Non-small cell lung cancer tumors of squamous histology.
T Cells – T cells are a type of white blood cell that is a component of the immune system that, in general, fights against infection and harmful cells like tumor cells.11
Tetravalent – A tetravalent molecule has four binding sites or regions.
Tumor Microenvironment – The tumor microenvironment is the ecosystem that surrounds a tumor inside the body. It includes immune cells, the extracellular matrix, blood vessels and other cells, like fibroblasts. A tumor and its microenvironment constantly interact and influence each other, either positively or negatively.12
VEGF – Vascular Endothelial Growth Factor is a signaling protein that promotes angiogenesis.13
6 Shibuya M. Vascular Endothelial Growth Factor (VEGF) and Its Receptor (VEGFR) Signaling in Angiogenesis: A Crucial Target for Anti- and Pro-Angiogenic Therapies. Genes Cancer. 2011 Dec;2(12):1097-105.
7 Stefan MI, Le Novère N. Cooperative binding. PLoS Comput Biol. 2013;9(6)
8 US National Cancer Institute, a part of the National Institute of Health (NIH). https://www.cancer.gov/about-cancer/treatment/types/immunotherapy. Accessed October 2023.
9 Han Y, et al. PD-1/PD-L1 Pathway: Current Researches in Cancer. Am J Cancer Res. 2020 Mar 1;10(3):727-742.
10 Han Y, et al. PD-1/PD-L1 Pathway: Current Researches in Cancer. Am J Cancer Res. 2020 Mar 1;10(3):727-742.
11 Cleveland Clinic. https://my.clevelandclinic.org/health/body/24630-t-cells. Accessed October 2023.
12 MD Anderson Cancer Center. https://www.mdanderson.org/cancerwise/what-is-the-tumor-microenvironment-3-things-to-know.h00-159460056.html. Accessed October 2023.
13 Shibuya M. Vascular Endothelial Growth Factor (VEGF) and Its Receptor (VEGFR) Signaling in Angiogenesis: A Crucial Target for Anti- and Pro-Angiogenic Therapies. Genes Cancer. 2011 Dec;2(12):1097-105.